


Intramuscular Injections Are Safer Procedures


Intramuscular Injection Information and Procedures
Both Testosterone and Human Growth Hormone Replacement Therapy can be delivered through injection. Although Testosterone can be delivered in multiple ways, including patch, spray, cream, and dermal implant, many people prefer to deliver the hormone via injection.
Even though HGH and Testosterone can be administered using a needle, they are injected differently. Whereas HGH is injected beneath the skin using an insulin needle, Testosterone is delivered directly into the muscle using a method known as Intramuscular Injection.
This article will more fully explain Intramuscular Injections, and it will also describe the actual protocol used for injection.
Why Do We Deliver Some Medicines Intramuscularly?
Intramuscular Injections are Safer
There are many reasons why some medications are delivered Intramuscularly, as compared to Intravenously or Subcutaneously. Compared to Intravenous Injections, Intramuscular Injections are considered safer than Intravenous Injections.
Intramuscular Injections are Easier
In addition, Intramuscular Injections are much easier to perform than Intravenous Injections. With an Intravenous Injection, it is necessary to target and hit a vein to deliver the medication. This is easier for some patients than others.
Some patients have deeper veins that are harder to target, and others have rolling veins that shift as the needle pierces the skin, making it hard to find the vein with a needle.
Intravenous Injections can Cause Damage.
Intravenous Injections can also damage the veins, whereas muscle fibers are constructed in a way where the damage caused by injection is negligible. Intramuscular and Subcutaneous Injections are more accessible and safer to perform than Intravenous Injections. Intravenous Injections are generally preferred for drugs that "drip" into the system, meaning that they supply a slow and constant supply of medication into the bloodstream.
Intramuscular Injections are Fast Acting, but Release Can Be Controlled
Intramuscular Injections act faster than Subcutaneous Injections but still deliver the medication to the body for a number of hours. Many drugs used via Intramuscular Injection, like Testosterone Hormone Replacement Therapy, contain ester compounds to slow the release of medication into the bloodstream. Ester compounds have relatively long half-lives and release Testosterone slowly over time.
Some Testosterone Esters break down entirely over a relatively brief period, only a few days. Other Testosterone Esters, like Testosterone Cypionate 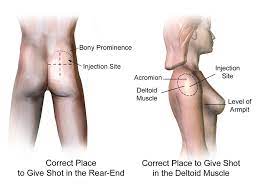 and Testosterone Enanthate, take one-to-two weeks to release the entire dose into the bloodstream. This is one reason many patients choose Testosterone Injections over less invasive methods.
and Testosterone Enanthate, take one-to-two weeks to release the entire dose into the bloodstream. This is one reason many patients choose Testosterone Injections over less invasive methods.
Most popular Testosterone Shots only have to be delivered every week or two, whereas most other forms must be applied daily. Testosterone Dermal Implants deliver Testosterone for an even more extended period, but this treatment is much newer and less popular than other forms.
Do Intramuscular Injections Hurt?
The pain associated with the injection is considered slightly more significant than the pain associated with Intravenous Injection, but most users find the pain tolerable and quite bearable.
Where are Intramuscular Injections Delivered?
Intramuscular Injections are delivered into muscle tissue beneath the Subcutaneous layer underneath the skin. This muscle tissue is known as Striated tissue.
What Size of Needle is Used for Intramuscular Injection?
The needles used for Intramuscular injection are slightly larger than those used for Subcutaneous injection. The needles are usually 1-1.5 inches long and gauge between 19 and 22. Some specific muscles contain more striated muscle tissue than others, and these are considered the ideal location to perform Intramuscular Injection. These muscles are the muscles of the thigh (vastus lateralis), the upper arm (deltoids), and the buttocks (gluteal).
The gauge and length of the needle depend upon the amount of fat at the injection site. Individuals that have higher levels of body fat need longer needles than those that don't. If the needle is not long enough to pierce into the striated muscle tissue, the medication will be delivered into adipose fat tissue rather than the intended muscle.
This is a more significant issue with women than men because women biologically produce higher fat levels than men. Injections that are delivered into the body fat are known as Intralipomatous Injections. Suppose injections are accidentally delivered into fatty tissue.
In that case, this has the potential to severely restrict the ability of the medication to release into the body quickly and effectively because there are very few veins in fat tissue, which slows down the medication's dispersion.
Rotating injection Sites with Intramuscular Injections
When patients are required to undergo multiple Intramuscular Injections over a specific time, it is vitally important to change injection sites with every subsequent shot. Testosterone Injections are an example of a medical therapy that requires multiple shots, generally ranging from four per week to once every two weeks. Repeatedly performing injections into the same site can damage muscle tissue and cause skin tissue to weaken and pit as well.
Dosage Volumes with Intramuscular Injection
Like Subcutaneous Injections, Intramuscular Injections are intended for relatively small doses of medication. However, muscle tissue can effectively absorb and distribute a higher volume of medication without causing any significant issues. Subcutaneous Injections max out at a volume of 2 milliliters no matter where the shot is administered. For Intramuscular Injection, the maximum dosage depends on the size and location of the muscle chosen for injection.
Some muscles can accept less medication than others. The thighs and deltoids, for example, can only intake around two milliliters of medication, but the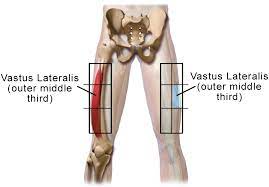 glutes can safely tolerate up to five milliliters of medication. Intramuscular injections are generally reserved for solid and potent medications and treatments, such as Sermorelin Acetate Therapy and Testosterone Hormone Replacement Therapy.
glutes can safely tolerate up to five milliliters of medication. Intramuscular injections are generally reserved for solid and potent medications and treatments, such as Sermorelin Acetate Therapy and Testosterone Hormone Replacement Therapy.
What Areas Should I Avoid When Injecting Intramuscularly?
When attempting to deliver your Intramuscular Medication, there are certain things you want to avoid. Delivering the injection far away from blood vessels and significant nerves is essential. If a needle clips a nerve, this will be very painful, and it will also do damage to the nerve. Nicking a blood vessel is bad because Intramuscular Injections are not intended for Intravenous application, and many intramuscular medications can be dangerous if injected into a vein.
Testosterone Injections, for example, are delivered via oil solutions so that they soak more readily into muscle tissue. Still, oil directly enters the bloodstream and can cause dangerous cardiovascular issues such as embolism or blockage.
Oil bubbles act like air bubbles or other physical obstructions in the bloodstream. It is straightforward to avoid this, however, because you will know if you hit a vein because blood will enter the syringe when you pull the plunger back. This process is known as aspiration.
You should also avoid any area of the skin which is irregular or damaged. Delivering an injection through a patch of skin that is infected can significantly increase the chance that you will experience a blood infection. You should also avoid scarred or irritated skin as well.
Side-Effects of Intramuscular Injection
If you experience any of the following issues as a result of Intramuscular Injection, discuss them with your doctor:
Scar Formation Can be avoided by rotating injection sites properly and performing injections carefully
Skin Sloughing Can be avoided by rotating injection sites properly
Hematoma Can be avoided by ensuring that injections are not delivered into veins
Embolism Can be avoided by ensuring that injections are not delivered into veins
Cysts Injecting too close to nerves can lead to cyst formation
Abscesses can occur as a result of infection. Always carefully sterilize all equipment, wash hands thoroughly, and clean the injection site
Why Choose Intramuscular Injections Over Intravenous Injections?
Although Intravenous Injections are the only choice for delivering large amounts of medication very quickly, Intramuscular Injections are ideal for delivering a small to moderate amount of medication over an extended period. One reason this is so is that Intramuscular Injections are released slowly by the muscle tissue into the blood supply.
When an Intramuscular Injection is delivered, it forms a deposit in the muscle tissue known as a Depot. This pocket of medication within the muscle tissue drains slowly into the bloodstream over time. Absorption rates depend upon multiple physiological factors, including circulation to the muscle, the depth at which the medication was injected, the type of drug formulation, and the amount of exercise the muscle receives.
How Formulations Affect Absorption
Intramuscular Injections are very versatile because they can be formulated to release into the body at various rates. The body metabolizes water/Saline Solutions at the fastest rate. Oil solutions take much longer to release into the body.
In addition, medications can be designed as colloids or suspensions in either oil or water formulations to increase the absorption rate further. Drugs can also be chemically combined with various salt forms to decrease solubility. This works exceptionally well within oil solutions because oil absorbs salt very slowly.
Drugs like Testosterone Cypionate and Testosterone Proprionate are attached to ester compounds, releasing them slowly over an extended period. Esters are very effective at providing a large number of dispersion rates because Esters Dissolve from their host into the bloodstream at a rate that is precisely correlated with the number of carbon molecules attached to the ester.
This means that Bio-Identical Testosterone can be released into the bloodstream over a day or the course of two weeks simply as a result of the size of the ester molecule.
What Type of Medications Are Delivered Intramuscularly?
Various forms of medication are delivered via the Intramuscular route, including:
Haldol
Ativan
Morphine
Codeine
Some many nutrients and hormones are delivered via Intramuscular Injection:
Progesterone
Testosterone
HCG
Vitamin B12
Plasma Injections
Many forms of vaccinations are delivered Intramuscularly. Including:
Flu Vaccines
Rabies Shots
Hepatitis A Vaccinations
HPV Inoculations
How To Perform an Intramuscular Injection
There are different sets of guidelines for how to deliver an Intramuscular Injection, depending upon the muscle you will inject the medication. Some muscles may require you to stretch the skin and bunch the muscle, whereas other locations may require you to stretch both the muscle and the skin. Some rules are universal, however:
Always wash your hands thoroughly before injection.
If someone else is delivering the injection, they should wear gloves.
Always disinfect the space in which you will perform the injection.
Always clean the injection site before injection.
Never use medication that is out of date.
Always store medications properly.
Administer the injection into the relaxed muscles to maximize effectiveness and minimize pain.
Always use a needle that is appropriate to the injection site.
Never let the tip of the needle make unnecessary contact.
When drawing medication, always release any air trapped within the needle by turning it upwards, tapping the syringe, and pressing the air out with the plunger until all bubbles are released. Injecting even a single air bubble is dangerous and can cause numerous complications.
Aspirate the needle slightly before injection to ensure that you have not hit a vein. If you have, you will have to adjust the injection site.
Always dispose of needles in an approved SHARPS container. Used needles are biohazardous waste and must be treated with extreme caution and care.
Intramuscular Injection into the Deltoid:
A second party must deliver deltoid Injections because it requires two hands to deliver the injection. This injection site is generally utilized for vaccinations and medications, which cause minor irritation. This location is intended for small amounts of medication ranging from 1-2 milliliters in volume. Deltoid Injections may not be an option for patients with very low muscle mass.
To choose an appropriate location for Deltoid Injection, start at the bone of the shoulder and move about an inch and a half beneath the process. This muscle is triangular, with its widest portion at the top of the muscle. Inject into an area at or near the thickest part of the muscle, which is in the center of  the triangle.
the triangle.
It is essential to inject in the central portion of the muscle because the Radial Nerve and Brachial Artery are located just on the outer edge of the Deltoids.
For this location, stretch out the skin and grip down around the muscle, squeeze your fingers together so that the skin remains tight, but you have squeezed the muscle. Insert the needle into the muscle at a 90-degree angle.
Intramuscular Injection into the top of the Thigh (Vastus Laterus):
This location disperses medication quicker than the buttocks but slower than the deltoids. The appropriate location to inject into the top of the thigh is between one hand-width beneath the groin and one hand-width above the knee. In this window, choose a location near the thickest part of the muscle.
Thigh injections are often preferred by individuals who self-inject because it is easy to access the thigh muscle from a prone or sitting position.
Stretch the skin tightly to reduce the distance that the needle must travel. Insert the needle directly into the muscle at a right angle to the leg. You can deliver up to two milliliters of medication per injection at this location.
Intramuscular Injection into the Hip (Ventrogluteal):
The Ventrogluteal site is widely considered the best location to deliver an intramuscular injection, either via self-administration or via the assistance of a second party. This location represents the thickest portion of the glutes, as this area includes both the Gluteus minimus and the Gluteus medius. This area also has some of the thinnest layers of fat tissue anywhere in the gluteal region.
It is also the safest area to deliver injection because there are no veins or nerves in range of the needle in this area, so you are primarily attempting to avoid bone. It is safe to deliver up to two milliliters of medication using this injection site.
Locate the outer protrusion of the upper femur, known as the prochanter. Then locate the protrusion of the hip bone, known as the Iliac Crest. Move your hand forward until you reach the crest point furthest from the center. This is known as the Anterior Iliac Crest.
You will deliver the injection at a point equidistant from both of these protrusions. Laterally, the injection site will be located halfway between the crest's center and the front. In your mind, this should form an upside-down triangle.
Aim for a location in the center of the triangle, equally far away from both bones. Tighten the skin around the injection site, then deliver the needle directly into the muscle at a 90-degree angle.
Intramuscular Injection into the Buttock (Gluteus medius):
In this location, injections can only be administered by a second party. This location is ideal for larger injections of up to five milliliters. You must be very careful when delivering an injection to this location because the superior gluteal artery and the sciatic nerve are only about three centimeters away from the injection site, making it vitally important that the injection is delivered to the correct location based on physiological landmarks.
Every time this injection is performed, it is essential to physically locate both the Posterior Iliac Crest and the Trochanter. This area also has a large amount of fat and requires longer needles than many other sites. The amount of fat tissue also slows down absorption, which should be considered when choosing this location.
Locate the protrusion of the upper femur, known as the trochanter. Then, locate the Posterior Iliac Crest. Place your hand on the central portion of the protrusion of the hipbone and move your hand back until you reach the portion of the bone furthest from the median. You may notice that many individuals have dimples located directly above this bone.
Imagine that there is a line that stretches directly from the Posterior Iliac Crest to the Trochanter. Move to the center of this line, then follow the line one inch further upward. This is the ideal injection site. Stretch the skin taut and deliver the needle directly into this point at a 90-degree angle.
- 0001) What Are Normal Testosterone Levels For Men And Women Throughout Life? [Last Updated On: February 14th, 2025] [Originally Added On: May 26th, 2020]
- 0002) Top Tips For Boosting Testosterone Naturally [Last Updated On: September 27th, 2025] [Originally Added On: May 27th, 2020]
- 0003) The Testosterone Factor [Last Updated On: October 28th, 2025] [Originally Added On: May 28th, 2020]
- 0004) Testosterone Can Help Relieve The Menopause Symptom Of Hot Flashes [Last Updated On: February 14th, 2025] [Originally Added On: May 29th, 2020]
- 0005) How Does Low Testosterone Cause Infertility? [Last Updated On: February 2nd, 2026] [Originally Added On: May 30th, 2020]
- 0006) The Benefits Of Testosterone Therapy For Prostate Cancer [Last Updated On: February 14th, 2025] [Originally Added On: May 31st, 2020]
- 0007) Is Testosterone Replacement A Valid Diabetes Treatment? [Last Updated On: February 15th, 2025] [Originally Added On: June 1st, 2020]
- 0008) Testosterone Shock Therapy May Be An Effective Prostate Cancer Treatment [Last Updated On: January 24th, 2026] [Originally Added On: June 2nd, 2020]
- 0009) Testosterone Replacement Therapy Is Safe For The Heart [Last Updated On: February 14th, 2025] [Originally Added On: June 3rd, 2020]
- 0010) Testosterone Replacement Therapy [Last Updated On: October 22nd, 2025] [Originally Added On: June 4th, 2020]
- 0011) Testosterone Patches [Last Updated On: February 1st, 2026] [Originally Added On: June 5th, 2020]
- 0012) Testosterone Overview [Last Updated On: February 13th, 2025] [Originally Added On: June 6th, 2020]
- 0013) Testosterone Levels And Making Money [Last Updated On: September 10th, 2025] [Originally Added On: June 7th, 2020]
- 0014) Testosterone Enanthate [Last Updated On: September 9th, 2025] [Originally Added On: June 8th, 2020]
- 0015) Increased Awareness Of Low-t Helps Men Live Healthier Lives [Last Updated On: January 31st, 2026] [Originally Added On: June 9th, 2020]
- 0016) How Does Low-t Lead To Erectile Dysfunction? [Last Updated On: January 30th, 2026] [Originally Added On: June 10th, 2020]
- 0017) Testosterone Basics [Last Updated On: January 27th, 2026] [Originally Added On: June 11th, 2020]
- 0018) How Does Testosterone Impact Prostate Health? [Last Updated On: January 26th, 2026] [Originally Added On: June 12th, 2020]
- 0019) Testosterone And Other Sex Hormones Impact Asthma Response Dependent On Sex [Last Updated On: January 23rd, 2026] [Originally Added On: June 13th, 2020]
- 0020) Recognizing Subtle Symptoms Of Testosterone Deficiency [Last Updated On: January 22nd, 2026] [Originally Added On: June 15th, 2020]
- 0021) Testosterone Trivia [Last Updated On: January 21st, 2026] [Originally Added On: June 16th, 2020]
- 0022) The Health Benefits Of Testosterone And Sleep Are Interconnected [Last Updated On: January 20th, 2026] [Originally Added On: June 17th, 2020]
- 0023) How Can I Restore My Testosterone Production Naturally? [Last Updated On: September 4th, 2025] [Originally Added On: June 18th, 2020]
- 0024) Low-t Quiz [Last Updated On: September 3rd, 2025] [Originally Added On: June 19th, 2020]
- 0025) Low Testosterone Might Mean Poor Sleep Need Testosterone Hormone Injections [Last Updated On: September 2nd, 2025] [Originally Added On: June 20th, 2020]
- 0026) Low Testosterone Contributes To Frailty With Age [Last Updated On: September 1st, 2025] [Originally Added On: June 21st, 2020]
- 0027) Low Testosterone Affects A Third Of Young Men With Type 2 Diabetes [Last Updated On: August 31st, 2025] [Originally Added On: June 22nd, 2020]
- 0028) Japanese Testosterone Study Proves Physical And Psychological Benefits [Last Updated On: August 30th, 2025] [Originally Added On: June 23rd, 2020]
- 0029) Injecting Testosterone (im) [Last Updated On: October 24th, 2025] [Originally Added On: June 25th, 2020]
- 0030) Injectable Testosterone And Testosterone Cream [Last Updated On: February 14th, 2025] [Originally Added On: June 26th, 2020]
- 0031) Indiana Jones Vs. Rambo (hgh Testosterone) [Last Updated On: August 28th, 2025] [Originally Added On: June 27th, 2020]
- 0032) How Much Does Testosterone Control Men's Behavior? [Last Updated On: August 27th, 2025] [Originally Added On: June 28th, 2020]
- 0033) Getting To The Bottom Of Low-t Under-reported Sources Of Testosterone Deficiency [Last Updated On: February 14th, 2025] [Originally Added On: June 29th, 2020]
- 0034) How To Manage And Overcome Testosterone Deficiency [Last Updated On: August 26th, 2025] [Originally Added On: June 30th, 2020]
- 0035) Clomiphene Low-testosterone Andropause Treatment [Last Updated On: January 19th, 2026] [Originally Added On: July 1st, 2020]
- 0036) How Do Synthetic Chemicals Impact Testosterone Secretion? [Last Updated On: August 18th, 2025] [Originally Added On: July 2nd, 2020]
- 0037) Interest In Bio-identical Testosterone Is Skyrocketing [Last Updated On: August 25th, 2025] [Originally Added On: July 3rd, 2020]
- 0038) Axiron Spray-application Testosterone Replacement Therapy [Last Updated On: August 24th, 2025] [Originally Added On: July 4th, 2020]
- 0039) Andropause: Male Menopause [Last Updated On: September 14th, 2025] [Originally Added On: July 5th, 2020]
- 0040) Testosterone Deficiency Treatment Options [Last Updated On: August 21st, 2025] [Originally Added On: July 6th, 2020]
- 0041) The Facts About Testosterone Hrt For Low-t [Last Updated On: August 22nd, 2025] [Originally Added On: July 7th, 2020]
- 0042) Misconceptions About Testosterone Replacement Therapy [Last Updated On: August 23rd, 2025] [Originally Added On: July 8th, 2020]
- 0043) Testosterone Replacement Therapy Facts And Myths [Last Updated On: October 4th, 2025] [Originally Added On: July 9th, 2020]
- 0044) Testosterone Injections For Testosterone Deficiency [Last Updated On: September 18th, 2022] [Originally Added On: July 10th, 2020]
- 0045) Testosterone Replacement Therapy May Help Aging Males Prevent Diabetes [Last Updated On: August 19th, 2025] [Originally Added On: July 11th, 2020]
- 0046) The Benefits Of Testosterone Replacement Therapy For Women [Last Updated On: August 17th, 2025] [Originally Added On: July 13th, 2020]
- 0047) How Can Testosterone Hrt Improve My Life Via Quality Low-t Treatments [Last Updated On: September 13th, 2025] [Originally Added On: July 14th, 2020]
- 0048) Frequently Asked Questions About Testosterone [Last Updated On: August 20th, 2025] [Originally Added On: July 15th, 2020]
- 0049) Bio-identical Testosterone Cypionate Injections [Last Updated On: August 16th, 2025] [Originally Added On: July 16th, 2020]
- 0050) All About Testosterone Creams [Last Updated On: August 13th, 2025] [Originally Added On: July 17th, 2020]
- 0051) Low Testosterone Treatment Protocols [Last Updated On: April 1st, 2025] [Originally Added On: July 19th, 2020]
- 0052) Testosterone Deficiency Drains Your Energy [Last Updated On: February 13th, 2025] [Originally Added On: July 21st, 2020]
- 0053) What Is Testosterone? [Last Updated On: August 11th, 2025] [Originally Added On: July 23rd, 2020]
- 0054) Eleven Signs Of Testosterone Deficiency [Last Updated On: March 30th, 2025] [Originally Added On: July 26th, 2020]
- 0055) Hypertension-Associated Cardiovascular Risks Increase Due To Both Low-T And High Testosterone [Last Updated On: February 18th, 2025] [Originally Added On: April 22nd, 2021]
- 0056) Everything to Know About Androgel [Last Updated On: March 27th, 2025] [Originally Added On: July 8th, 2021]
- 0057) Kinds of Testosterone Therapy – Which Is Right for You? [Last Updated On: March 21st, 2025] [Originally Added On: August 28th, 2021]
- 0058) This Study Says High Protein Diet May Suppress Testosterone Levels [Last Updated On: February 20th, 2025] [Originally Added On: March 28th, 2022]
- 0059) Testosterone and Estrogen Deficiency Associated With Increased Risk of Rotator Cuff Surgery [Last Updated On: February 14th, 2025] [Originally Added On: April 26th, 2022]
- 0060) Low Testosterone Accelerates Aging [Last Updated On: March 20th, 2025] [Originally Added On: May 3rd, 2022]
- 0061) Low Testosterone Endangers Your Health [Last Updated On: February 14th, 2025] [Originally Added On: May 14th, 2022]
- 0062) Testosterone Helps Modulate Immune Activity in the Digestive System [Last Updated On: February 14th, 2025] [Originally Added On: May 18th, 2022]
- 0063) Did you know: Testosterone treats depression! [Last Updated On: November 6th, 2025] [Originally Added On: May 19th, 2022]
- 0064) Benefits of Fenugreek – Boost Testosterone and More [Last Updated On: February 14th, 2025] [Originally Added On: May 23rd, 2022]
- 0065) Testicle Tanning: What is Tucker Carlson Talking About? [Last Updated On: April 16th, 2025] [Originally Added On: June 3rd, 2022]
- 0066) Using Testosterone to Combat Memory Issues in Diabetics [Last Updated On: February 14th, 2025] [Originally Added On: August 16th, 2022]
- 0067) About 40% of Men Have Low-T – and it Doubles the Risk of Severe COVID [Last Updated On: February 25th, 2025] [Originally Added On: September 21st, 2022]
- 0068) The Foods To Boost Your Testosterone…And The Foods To Avoid [Last Updated On: November 4th, 2025] [Originally Added On: September 30th, 2022]
- 0069) Tlando Testosterone: An Innovative Oral Therapy for Low-T [Last Updated On: November 3rd, 2025] [Originally Added On: October 1st, 2022]
- 0070) Testosterone Replacement Therapy (TRT) Explained [Last Updated On: April 8th, 2025] [Originally Added On: October 12th, 2022]
- 0071) Examining The Link Between Testosterone and Employability [Last Updated On: February 18th, 2025] [Originally Added On: November 8th, 2022]
- 0072) Standard Measure of Low Testosterone Doesn't Apply to Young Men [Last Updated On: March 12th, 2025] [Originally Added On: November 8th, 2022]
- 0073) Surprising Things that Cause Men’s Crashing Testosterone [Last Updated On: March 17th, 2025] [Originally Added On: January 5th, 2023]
- 0074) Understanding the Correlation between Testosterone Levels and Job Performance [Last Updated On: February 9th, 2025] [Originally Added On: February 9th, 2025]
- 0075) Link between Low Testosterone and Severe COVID Symptoms in Men [Last Updated On: February 12th, 2025] [Originally Added On: February 12th, 2025]
- 0076) The Good Job Grip: Is Testosterone the Key? [Last Updated On: February 13th, 2025] [Originally Added On: February 13th, 2025]
- 0077) Importance of Nutritional Balance in a Healthy Diet [Last Updated On: February 14th, 2025] [Originally Added On: February 14th, 2025]
- 0078) Invigorating Power of the Fenugreek Plant: A Natural Testosterone Energizer and More [Last Updated On: February 14th, 2025] [Originally Added On: February 14th, 2025]
- 0079) Unlocking the Testosterone Treasure: A Panacea for Cognitive Woes in Diabetic Patients [Last Updated On: February 14th, 2025] [Originally Added On: February 14th, 2025]
Word Count: 2629
